The Clinical Data Interchange Standards Consortium (CDISC) is a global not-for-profit organisation that develops standards to support the acquisition, exchange, submission, and archive of data in clinical research. For pharmacokinetic (PK) analysis, those standards help structure how concentration results, derived parameters and analysis-ready datasets are prepared for review.
An important component of many clinical studies is the collection of Pharmacokinetic (PK) blood samples and the subsequent analysis of PK data. Pharmacokinetics studies how a drug is absorbed, distributed, metabolised and excreted (ADME) over time. By analysing PK data, efficacy and toxicity outcomes can be improved for patients and better understood in relation to drug exposure. The CDISC standards most associated with the analysis and submission of PK data are the Study Data Tabulation Model (SDTM) and Analysis Data Model (ADaM). This guide explains how PK data typically move from source data into SDTM PC and PP, then into ADPC, ADPP and final tables, listings and figures.
In Brief
- CDISC compliant PK Analysis means organising concentration results, derived parameters and analysis datasets so PK data can be reviewed clearly.
- In clinical development, this matters because PK findings help interpret drug exposure in relation to efficacy, toxicity and dose decisions.
- Operationally, PK data move through CRF/eCRF records, bioanalytical transfers, SDTM PC and PP, ADPC, ADPP and final TLFs.
- A common risk is assuming SDTM PC can be used directly for PK parameter derivation without the added timing, dosing and analysis variables needed in ADPC.
- The main takeaway is that timing rules, unit handling, BLQ/LOQ decisions and traceability should be defined early and documented consistently.
PK data sources and identifiers for CDISC workflows
PK data can be found in the CRF/eCRF, which is collected at the study site, or through bioanalytical lab data, which is processed externally. The CRF/eCRF will often include sample collection dates and times, dosing details and visit information, while the bioanalytical transfer will usually contain concentration results, analyte names, specimen types, units and laboratory sample identifiers. PCREFID can be used in SDTM to store specimen identifiers from these sources. Other identifiers may also be needed to align subject, specimen type, analyte, sample matrix, nominal timepoint, actual collection time and dosing reference. These joins should be considered early, because the same identifiers often support later traceability between PC, PP, ADPC and ADPP.
PK data in SDTM: PC for concentrations, PP for parameters
There are two primary SDTM domains dedicated to the submission of PK data: the Pharmacokinetic Concentration (PC) domain and the Pharmacokinetic Parameter (PP) domain.
PC is a findings domain used for the submission of all concentration results (from samples such as plasma and urine) of drugs and metabolites as a function of time. It has a structure of one record per subject/dose/day/analyte/time point, hence concentration-time profiles are stored across multiple records. The PC domain ultimately forms the basis of the pharmacokinetic analysis used to derive multiple pharmacokinetic parameters for each individual Pharmacokinetic (PK) profile (such as Cmax, tmax, AUC, half-life, etc), which are subsequently submitted in the Pharmacokinetic Parameter (PP) domain.
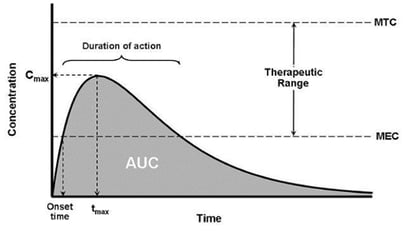
Figure 1: PP parameters tmax, Cmax and AUC
PP is a findings domain containing PK parameters derived from PC data. It has a structure of one record per PK parameter per concentration-time profile, and although the data presented are not observed data, the submission of PK Parameters fits well into the SDTM general observation class model. This distinction is important because PC preserves the concentration-time observations, while PP presents the derived results from those profiles. Reviewers need to be able to understand both datasets and the relationship between them.
Timing and merges
Timing and unit decisions for calculating each parameter should be consistent and documented by the sponsor. While nominal timings for measurements will be documented in the protocol, the actual times might slightly differ, and these should also be recorded for accurate calculation of PP parameters. Actual elapsed time is often calculated relative to a dosing reference, so the dosing date/time, sample collection date/time and reference timepoint should be aligned clearly.
Unit choices need the same level of control. Concentration, dose, urine volume, elapsed time and parameter units should either be standardised or handled through documented conversion logic. Where the bioanalytical dataset, CRF/eCRF and analysis software use different conventions, the selected standard units should be visible in the dataset specifications and supporting metadata.
From SDTM to analysis: ADPC and ADPP essentials
Generating SDTM PP domains from SDTM PC domains is not quite as simple as it may seem. PK analyses typically require a number of variables which cannot be added to the SDTM PC domain (such as dose level, actual time relative to dosing, etc); therefore, it is not possible to simply feed SDTM PC into an appropriate software package (such as Phoenix WinNonlin) and generate derived PP data. In order to do this, an intermediate analysis dataset must be produced, and this is where ADaM provides the structure of analysis-ready PK data.
ADaM standards allow SDTM datasets to be transformed for analysis purposes, and should typically be ‘one procedure away’ from an output. The analysis of PK data generally involves the creation of two separate ADaM datasets: ADPC and ADPP. ADPC typically contains all relevant variables from SDTM PC, merged with ADSL (i.e. the primary subject level data such as demography and treatment information), EX (for dose information), and including additional variables required for the PK analysis (such as the actual time relative to the start of dosing for each PK profile). Depending on the study, ADPC may also include analysis flags, standardised analysis values, elapsed time variables and other variables specified in the protocol, statistical analysis plan or PK analysis plan. ADPC can then be fed directly into Phoenix WinNonlin (or alternative PK software packages) to derive the Pharmacokinetic (PK) parameters. These parameters are subsequently used to populate the SDTM PP domain, which in turn is merged with ADSL to create ADPP, the PK analysis dataset used in the statistical analysis of PK data (such as dose-proportionality and bioequivalence analyses).
BLQ/LOQ handling and common edge cases
For analysis and summary statistics, BLQ (below limit of quantification) records should be dealt with in a pre-specified manner, for example setting as half of the LLOQ (lower limit of quantification). This is only one possible approach; the selected BLQ and LLOQ handling rules should be defined in the statistical analysis plan, PK analysis plan or data handling specification and then applied consistently.
In preparation for the creation of PP from PC, for urine samples, start and end times for the sampling interval should be created in ADPC. Urine analyses may also need clear alignment between concentration, collection interval and volume records.
Multiple analytes, multiple matrices/sample types, repeated profiles and mixed units should be resolved through documented mapping rules rather than late-stage programming assumptions.
Traceability patterns regulators expect
Once the SDTM and ADaM datasets have been created there is one more important consideration when submitting PK data in CDISC format, and that is the requirement to link all derived PP parameters back to the original PC observations. This link can be established through RELREC or documented through ADaM analysis datasets/metadata. The purpose is to show which concentration records were used to calculate each PK parameter.
The primary method to link PP and PC observations which is detailed in the SDTM IG (Study Data Tabulation Model Implementation Guide) is a RELREC table. The general concept of RELR EC tables is that related records from each domain are presented in adjacent rows, with variables (such as IDVAR, IDVARVAL and RELID) used to link each observation together. In RELREC, records can be linked using a pair of PCSEQ, PCGRPID, PPSEQ and PPGRPID depending on whether individual records or a group of records should be linked to each other (this is a choice of prioritising fewer RELREC records or not needing to derive GRPID for PC and/or PP domains).
However, the submission of records in RELREC can vary in complexity a great deal, and for this reason many sponsors prefer to link PC and PP records using the analysis metadata. As a result, the SDTM IG also states that sponsors may document those concentrations used to calculate each PK parameter via the analysis datasets (i.e. ADaM). Whichever method is used, the linking logic should be documented clearly enough for a reviewer to follow the path from PP parameter back to the relevant PC profile.
Illustrative flow: CRF/BA → PC/PP → ADPC/ADPP → TLFs
An example workflow incorporating SDTM and ADaM datasets in a typical CDISC compliant Pharmacokinetic (PK) analysis is illustrated in Figure 2.
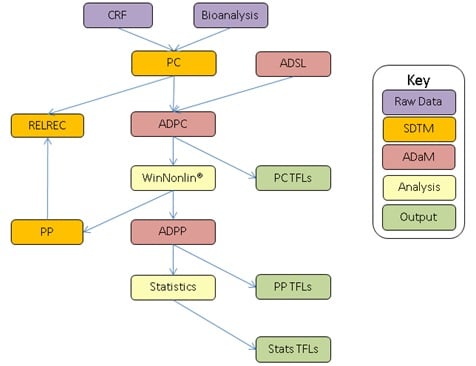
Figure 2: Example of SDTM and ADaM workflow associated with the submission of CDISC compliant PK datasets
SDTM: Study Data Tabulation Model, ADaM: Analysis Data Model, CRF: Case Report Form data, Bioanalysis: Bioanalytical results dataset, WinNonlin: PK analysis software, TFLs: Tables, figures and listings.
Regulatory positioning and practical checklist
To reduce avoidable review questions or technical issues, sponsors should follow applicable CDISC standards and document the main data handling decisions. Documentation is key to following the complex transformation of PK data from raw data to analysis, and traceability and logic used should be clear to the reviewer. Parameters should follow CDISC naming conventions and controlled terminology where applicable.
A simple checklist can help keep the package consistent:
Do:
-
Confirm how CRF/eCRF and bioanalytical records will be joined
- Document nominal and actual timing rules
- Standardise or document unit conversions
- Pre-specify BLQ/LOQ handling
- Maintain traceability between PP parameters and PC concentrations
Don't:
-
Leave sample identifiers unresolved until late programming
- Mix units without documented conversion logic
- Apply different BLQ rules across outputs without explanation
- Submit derived parameters without a clear link back to source profiles
Conclusion
CDISC standards have been in place for a number of years to streamline the submission of clinical study data, and are expected for many electronic regulatory submissions, including FDA submissions where applicable. CDISC compliant pharmacokinetic workflows are therefore important for sponsors preparing PK data for review.
FAQs
What is the difference between SDTM PC and PP?
PC contains PK findings as recorded with record(s) for each timepoint, while PP is derived from PC data with each time profile grouped into one parameter.
What are ADPC and ADPP, and when are they used?
ADPC is derived from PC with added variables to assist with the derivation of PP, and added variables for analysis. ADPP is derived from PP with added variables for analysis. ADPC is generally used to support concentration analysis and PK parameter derivation, while ADPP supports analysis and reporting of the derived parameters.
How do I link PK parameters back to source concentrations?
PK parameters can be linked back to source concentrations through the RELREC dataset or analysis metadata. The chosen method should identify which PC records contributed to each PP parameter.
What is the difference between nominal and actual time in PK data?
The nominal time is the planned time as per protocol for the PK sample to be taken, the actual time is when the sample was recorded to be taken. Both may be needed because PK parameters are often sensitive to the timing used in the calculation.
How should BLQ/LOQ values be handled?
BLQ/LOQ values should be handled in a consistent way as pre-specified in the SAP. The method should be documented before analysis and applied consistently across relevant datasets and outputs.
Quanticate’s statistical programming team can support clinical trial teams with CDISC compliant PK analysis workflows, from SDTM PC and PP datasets through to ADPC, ADPP, TLFs and submission-ready outputs. Our experts help sponsors build validated, traceable and well-documented programming processes, with clear handling of timing, units, BLQ/LOQ rules and PK parameter traceability. To discuss how we can support your clinical trial, request a consultation below.